


October POCUS Round Up
POCUS for pulse checks, diuretic response, increased ICP, head and neck applications, acute dyspnea, and PE eval in the ICU

Slipped into December and here I am with notes on 6 more papers from October, so here are some quick hits with links in case you’re interested.
The CLOSED protocol to assess optic nerve sheath diameter using color-Doppler: a comparison study in a cohort of idiopathic normal pressure hydrocephalus patients.
single center cross sectional cohort; included patients > 18 with suspected idiopathic normal pressure hydrocephalus
POCUS compared to MRI, images obtained right around the same time, POCUS performed in B mode (27 patients) or B mode with Doppler (23 patients)
the optic nerve sheath diameter (ONSD) was measured 3 mm behind the optic disc, all measures were bilateral in 2 planes, US performed by expert neurosonologist supported by an additional expert
50 consecutive patients, mean age 76 +/- 8 years
agreement between MRI and US relatively poor, color Doppler measures were less scattered and lower on average than B mode measures
The idea of using Doppler hadn’t honestly ever occurred to me for ONSD measurement, but the authors explain the rationale in their earlier paper outlining the CLOSED protocol: “[central retinal artery and vein] visualization helps to correctly identify the [optic nerve] course, which can be difficult due to artifacts, wrong angulation of the probe, and nerve tortuosity [15,16,17]. Furthermore, identifying the ophthalmic artery (OA) with color Doppler, which runs parallel to the [optic nerve], increases accurate identification of ONSD margins.”

Unfortunately, it doesn’t look like ultrasound performed well relative to MRI, even when performed by ‘expert neurosonologists’. Here’s Figure 3 from their paper summarizing the comparisons between imaging modalities:

I’d also be remiss if I didn’t point out that there are several spots where they don’t capitalize ‘Doppler’, which drives my former fellowship director batty (s/o @sono4pyro).
Point-of-care ultrasound in the head and neck region.
This was mostly just a review of H&N applications. I didn’t realize you could see the vocal cords and epiglottis! I think this would be a helpful application when trying to distinguish between upper and lower airway obstruction - this is especially tricky in kids sometimes whose already narrow upper airways don’t require the level of insult an adult airway might in order to cause respiratory distress.
Point-of-care ultrasound improves clinical outcomes in patients with acute onset dyspnea: a systematic review and meta-analysis.
13 studies included, 7 of which were RCT’s; lots of heterogeneity but a few really solid studies with low bias
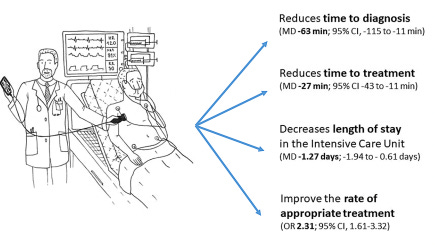
This article serves as a nice complement to the guideline on lung POCUS for the evaluation of acute dyspnea the ACP put out last year.
Diagnostic accuracy of multiorgan point-of-care ultrasound compared with pulmonary computed tomographic angiogram in critically ill patients with suspected pulmonary embolism.
Premise: prediction scores are inaccurate in the critically ill and they’re not always stable enough to head to the scanner for a CTA. Critically ill patients with suspected PE for whom a CTA was ordered were scanned by ICU fellows using a ‘standardized multiorgan POCUS’ exam including 2 point DVT study, lung ultrasound (to look for other explanation for signs/symptoms), and focused cardiac assessment. Fellows were blinded to CTA results and exams were performed within 24 hours of CTA.
37 of 88 patients had a PE: RV dysfunction (by TAPSE or RV/LV size ratio > or =1), no alternative diagnosis on Lung US, and D Dimer > 1000 had highest likelihood ratios —> when combined, all 3 findings had +LR 12.5 and -LR 0.52




This information will inform my illness script for PE moving forward and reinforces the need to examined the lung and right heart with ultrasound in the dyspneic or hypoxemic/hypoxic patient.
Point-of-care ultrasound compression of the carotid artery for pulse determination in cardiopulmonary resuscitation.
single center, prospective, cardiac arrest patients receiving CPR in the ED
carotid compression q2 minutes vs. manual palpation of femoral q2 minutes (during rhythm checks); POCUS carotid compression also q30 sec during compressions
median pulse check time with POCUS vs. palpation was 1.62 sec vs. 3.5 sec (which is insanely fast for both)
155 POCUS pulse checks in 25 patients, all under 10 seconds, only 5 took longer than 5 seconds (vs. five >10 sec and thirty-seven >5 sec in the palpation group)
in other studies the median manual pulse check time was 9.29 sec and 11.5 sec
Notably, they didn’t use doppler - technique was to orient a linear probe transverse to the carotid and apply pressure until the adjacent IJ was compressed. They looked for lack of pulsation and complete compression of the carotid as signs the pulse was absent. In brief, I think this is a cool, good idea that would be enhanced with use of color Doppler. Might allow for detection of ROSC while compressions are ongoing.
Doppler study of portal vein and renal venous velocity predict the appropriate fluid response to diuretic in ICU: a prospective observational echocardiographic evaluation.
prospective, observational study based in a CV/MedSurg ICU in Dijon, France; inclusion criteria were patients >18 with clinical signs of fluid overload, absence of response to passive leg raise, and for whom the treating doc had been trying loop diuretics for a few days
echo performed by expert
patients assigned ‘clinical congestion score’ from 0-10, > or = 3 was significant
score included pulmonary rales/crackles, peripheral edema, B lines, pleural effusion, and NTproBNP >1500
‘controls’ were assigned after the fact as patients whose baseline clinical congestion score was <3 or whose congestion score didn’t improve with diuretics (or who died)
primary outcome was score of < 3 after treatment/on last day in ICU; 34 experienced primary outcome out of 81 patients in experiment
portal pulsatility index (PPI = (Vmax - Vmin) / Vmax) and renal venous impedance (RVI = (peak systolic vel - end diastolic vel) / peak systolic vel) were better predictors of diuretic response than VEXUS, CVP, diuresis/natriuresis, and echo measures of left/right heart failure
It was weird to me how they chose to describe a control and treatment group when patients weren’t randomized or even assigned to one group or the other, just cherry picked after the fact based on whether or not their congestion score improved. Regardless, fluid overload and diuresis are hot topics in critical care right now, especially for patients with respiratory failure, and with a little practice these measures aren’t hard to snag. You just need a machine capable of pulse wave Doppler and the ability to image the portal veins and kidneys. Not entirely sure the juice is worse the squeeze, so to speak.