


Teach the Teachers and Boludo Pizza

“It’s easy to sit there and say you’d like to have more [POCUS].
And I guess that’s what I like about it.
It’s easy.
Just sitting there, rocking back and forth, wanting that [POCUS].”
Jack Handey
GME leaders are quick to cite a lack of trained faculty experts as reasons they don’t offer training for residents and interested faculty. They want to offer training, but *shrugs violently*. I came across this paper while doin research on a revision and wanted to write about it a bit along with a look at a kindred paper from 2017.
If you just want to read about pizza skip to the bottom.
Anstey J, Jensen T, Lalani F, Conner SM. Teaching the Teachers: A Flexible, Cognitive-Focused Curriculum in Point-Of-Care Ultrasound Education for Hospital Medicine Faculty. J Ultrasound Med. Published online September 5, 2022. doi:10.1002/jum.16091
PMID: 36063066
This was a cool paper out of the UCSF hospital medicine experience. In an effort to increase the number of POCUS-trained faculty they offered one of three pathways:
Educational Supervision (Harry Potter year 1): Complete five, 40-minute modules detailing an intro to POCUS, IVC evaluation, lung ultrasound, focused cardiac assessment, and abdominal ultrasound. All modules concluded with a case-based clinical integration piece. Estimated time to complete ~4 hours.
Limited Practice (David Blaine): participation in 4 image review sessions and at least 4 proctored scanning sessions OR a 1-day, 10 hour crash course that’s offered twice per year. Providers were also encouraged to complete the modules from the 1st path. Est time to complete ~10 hours.
Independent Practice (Gandalf the Grey): completion of both of the above plus an image portfolio (165 images), written exam (pass = 70%), and proctored skills assessment. Est time to complete ~40 hours.
They used handheld ultrasound probes with HIPAA compliant cloud for image archival (sounds like Butterfly IQ probs…) and offered the pathways to 116 hospitalists. 102 hospitalists engaged with the materials/pathways in some way and 55 completed at least one pathway with some crossover. This flowchart was helpful:
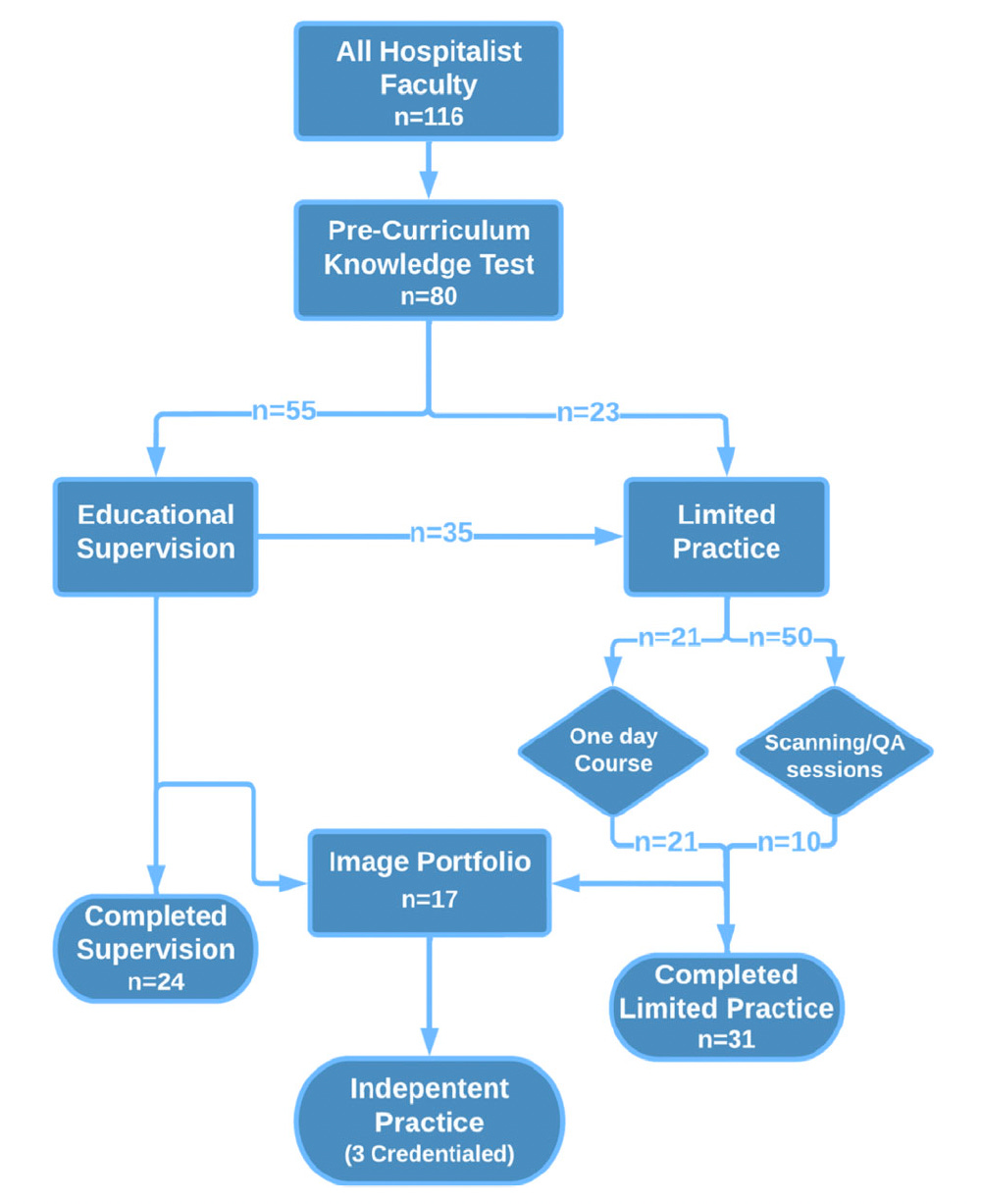
Notably, ‘senior’ hospitalists (>10 y in practice) demonstrated a significant preference (9 of the 11 participating) for the limited practice pathway, opting to have their first exposure to POCUS training a hands-on experience.
Takeaway: With a few POCUS champions and flexible pathways to competence, your institution can develop adept faculty with a reasonable time commitment. This is good for residents and faculty alike, and they might catch the bug seeking out additional training and CME. In particular, the educational supervision pathway, which is simply 4 hours of modules, would allow hospitalists to supervise residents performing POCUS. This is a good option for institutions with really limited means and no genuine POCUS wizards. The ACP has great modules that are free to members, so even that bit could be outsourced. It would leave you in the lurch a bit as regards quality assurance and maintenance of certification, but thankfully practical approaches to this have been described before…
Mathews BK, Zwank M. Hospital Medicine Point of Care Ultrasound Credentialing: An Example Protocol. J Hosp Med. 2017;12(9):767-772. doi:10.12788/jhm.2809
PMID: 28914285
Mathews and Zwank describe how hospitalists are credentialed and quality is assured in this paper from 2017. They describe forming a dream team at their hospital (read: POCUS committee) that did some research, came up with baseline training requirements and minimums for privileges, then developed standard image requirements for select exams and lobbied for a means of ordering and reporting in their EHR. Pays to have diverse stakeholders as buddies. Their committee was comprised of reps from hospital med, emergency med, critical care, radiology, and cardiology. They described 2 pathways:
Residency/Fellowship based: If you got 20 hours training including 6 hours hands on scanning and had at least 5 proctored limited cardiac exams + an image portfolio you could apply for credentials.
Practice Based: This pathway required 20 hours training to include at least 6 hours hands on + 5 proctored limited cardiac exams and a portfolio. Sound familiar?
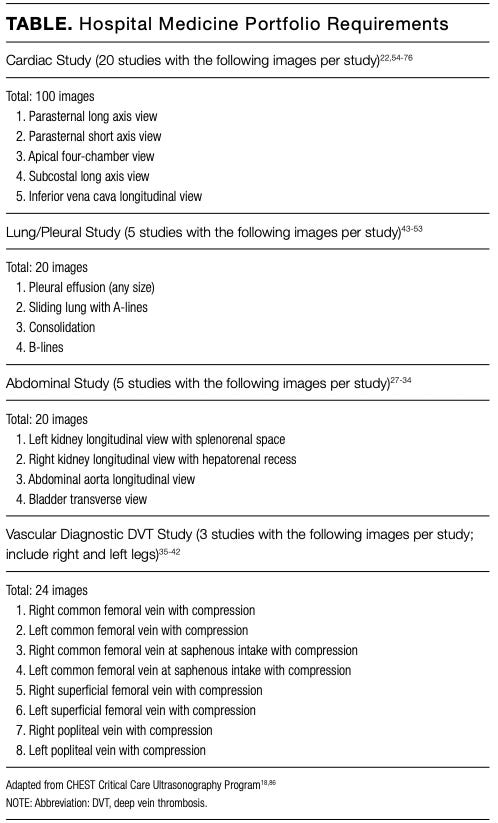
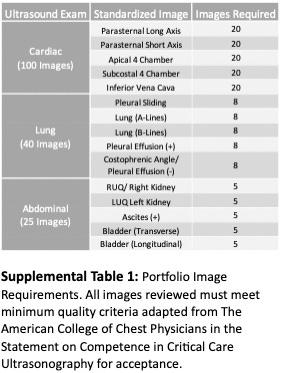
This table outlines minimum requirements. If you got 200 cardiac images but 150 were garbage you’ve still got 50 exams to record. The importance of something like a portfolio can’t be understated, and the authors point out it provides opportunities for assessment, feedback, and mentorship…so, coaching. Your own personal ultrasound Ted Lasso to gas you up, but also feed you reality sometimes. This is the model used (along with some in-person trainings) by CHEST and SHM for their certificates, which I believe to be gold-plated and individually numbered like commemorative coins.
Additionally, participants have to pass an exam with an 85% score. Anstey et al set the bar a little lower at 70%, because, after all, C’s do get degrees. I think 85% is a reasonable cutoff as long as the cases aren’t ambiguous in the least or participants are graded on thought process and reasoning in addition to hitting the mark.
Maintenance of certification would be achieved through at least 10 exams per year in each of the above domains (each cardiac window, lungs, abdominal, vascular). If a provider failed to hit 10 in a year then ALL their exams in that domain would be reviewed and they’d get an opportunity for supervised scanning to make up the difference.
Quality Assurance was performed at least quarterly on 10% of saved exams in each domain and images were always reviewed by at least 2 POCUS wizards - one hospitalist and one radiologist OR cardiologist depending on the exam. Exams were graded from 1 (stellar) to 5 (no bueno) with a 6 reserved for “unable to complete due to patient factors”. All 4s and 5s were reviewed at the quarterly POCUS Dream Team meetings.
They additionally mention that billing for POCUS exams is important to help offset the costs of implementing POCUS. Billing isn’t that hard, you just need retrievable images (so you need to save your exam) and a documented interpretation of findings. I like this page from POCUS 101 on billing codes and reimbursement.
Takeaway:
Step 1: Assemble interdisciplinary POCUS crew.
Step 2: Create matching embroidered denim jackets and/or vests.
Step 3: Create pathways for credentialing.
Step 4: Ensure processes for skill maintenance and quality assurance.
Step 5: Get paid.
Step 6: Buy pizza from Boludo in Minneapolis.
Boludo!
Their pizza is a spiritual experience. I’m having a hard time with all the unconscious saliva production going on in my mouth right now just thinking about it. Most of the pizzas are sort of a wood fired Italian style with relatively thin crust that’s both sturdy and chewy, somewhat charred round the edges. The Minneapolis Star Tribune critic called the chef a ‘dough whisperer’, which, aside from a difficult to navigate backside phoneme structure is apt AF. Look at this pie, my guy:

And the pepperonis do that thing where they form a cup when cooked - *shudders* so good. I dispatched one of these after a long run this past Saturday and felt a spiritual kinship with the winner of fat bear week, though my next move was to punish myself with 6 hours of scoreless baseball (the Astros will always be villains to me) and not a months long nap. I’ve also had the Peras pizza which features pear, gorgonzola, pine nuts, and dill. Would venture to say it’s even better than the pepperoni - one food critic from the cities called it ‘hall of fame worthy’, and I don’t know where the pizza hall is or if it exists but I know he’s right. Peep this pizza:

The dill garnishes this bad boy like Caesar’s coronet, crowning it king of pizzas. I’ve had one other pizza from Boludo and levy my only criticism at the profound amount of arugula they pile on top of it:

I promise there’s a pizza under there haha. This is the Sarandara, complete with tomato, prosciutto, fresh mozzarella, and did I mention the arugula? This pizza is a sweet deal if you were hoping for a pizza salad combo, but the salad does come on top of the pizza. Still delicious, and you’ll meet your daily fiber goals, just tough to navigate.
I’ve never been to Argentina and remain woefully ignorant of their pizza scene, but after eating at Boludo a handful of times it has moved up the list!
If you’re ever in town for a conference or a layover or a Vikings game, I can’t recommend Boludo highly enough. And please invite me to join you!